
Page 6 - reflections_dyslipidaemia_newsletter9_Final
P. 6
REFLECTIONS
Dyslipidaemia
Dyslipidaemia Global Newsletter #9 2025
The latest cholesterol guidelines advocate for CAC testing in individuals at intermediate risk when there is uncertainty about initiating
statin therapy for primary prevention. Studies have demonstrated that a CAC score can help reclassify ASCVD risk, potentially Dyslipidaemia
improving the risk prediction made by PCEs. For instance, a CAC score of 0 in adults with a 10-year calculated ASCVD risk of 5%
to <20% correlates with substantially lower actual event rates than predicted by PCEs alone, allowing reclassification to a lower risk
category. Furthermore, CAC screening has been shown to improve intermediary outcomes such as statin initiation and lower LDL-C
levels, suggesting that knowing one’s CAC score can enhance adherence to cardiovascular risk-reducing behaviours.
Despite its utility, CAC testing is not always appropriate. The authors review the evidence to consider when a CAC score
measurement is likely to be obtained too early, too late, or too often and then demonstrate these concepts and recommendations
through a series of case vignettes. Testing too early, particularly in individuals younger than 40–50 years, is generally not
recommended as a CAC score of 0 may provide false reassurance regarding long-term risk due to the later development of CAC
and a lack of validation in younger cohorts. For high-risk young adults with conditions like diabetes, a CAC score of 0 might be falsely
reassuring and should not delay appropriate statin use.
CAC testing can also be too late to be clinically helpful when an individual’s risk is already high enough that it wouldn’t warrant
a change in therapy, or when an older adult’s expected lifespan precludes time for benefit. Crucially, CAC measurement is not
recommended for patients already on statin therapy, as statins can paradoxically increase CAC levels due to plaque stabilisation
rather than plaque volume reduction, making it an unreliable marker for treatment efficacy or titration.
Finally, CAC testing can be performed too often, especially when it does not change clinical management. Current guidelines suggest
repeat imaging intervals of three to five years for individuals with a CAC score less than 100, or five to 10 years if the initial score was
0 without major risk factors. However, repeating CAC scores when the initial score is already high (e.g., ≥100 or ≥75th percentile) is
generally not beneficial, as intensive risk reduction with statin therapy is already warranted.
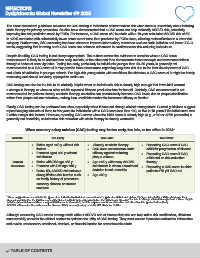
When coronary artery calcium (CAC) testing may be too early, too late, or too often in 2024 a
Variable Too Early Too Late b Too Often c
• Males aged <40 y without risk • Already on statin therapy • Repeating CAC score if CAC
factors • CAC does not measure statin ≥300 for progression of disease
• Females aged <50 y without efficacy against reducing • Repeating CAC score if CAC
risk factors plaque volume ≥100 and on risk-reduction
Clinical • Males with DM age <35 y • Age >65 y with many ASCVD therapy
Scenarios • Females with DM age <45 y risk factors in whom a treatment • Repeating a CAC score in older
• Below 5% ASCVD risk unless a decision is not uncertain patients >75 y if CAC = 0
strong lifetime risk burden such • Age ≥80 y
as family history of premature
coronary disease or current
smokers
a These suggestions cannot take the place of an individualised clinical assessment of a patient and their risk status. They are intended to aid the clinician in their
discussion of whether the CAC score test if obtained is likely to provide information that will change therapy. Too late to change clinical management. There may be
b
c
individual circumstances where a repeat CAC score is warranted, but this requires careful consideration and should not be performed routinely.
ASCVD, atherosclerotic cardiovascular disease; CAC, coronary artery calcium; DM, diabetes mellitus.
Although measuring CAC scores among adults without ASCVD and of intermediate risk can help refine risk stratification, clinicians
must carefully consider the clinical context to optimise the utility of CAC testing. They must ensure it provides actionable information
and avoids unnecessary emotional, physical, or financial burden for asymptomatic adults.
TABLE OF CONTENTS